
A hiatal hernia is a protrusion of a portion of the stomach through
the hiatus of the diaphragm and into the thoracic cavity.
Pathophysiology and Etiology
-
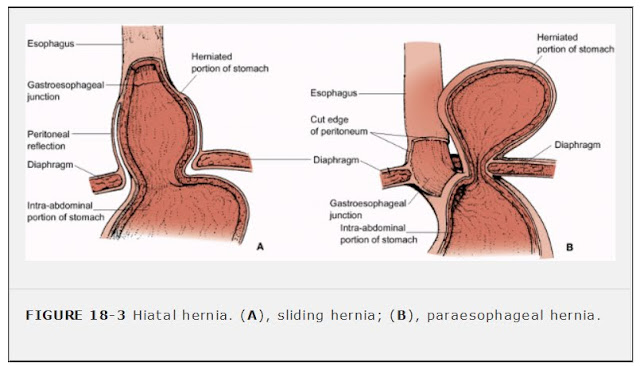
There are two types of hiatal hernias (see Figure 18-3):FIGURE 18-3 Hiatal hernia. (A), sliding hernia; (B), paraesophageal hernia.
-
Sliding hernia: Stomach and gastroesophageal junction slip up into the chest (most common)
-
Paraesophageal hernia (rolling hernia): Part of the greater curvature of the stomach rolls through the diaphragmatic defect
-
-
Caused by muscle weakening due to aging or other conditions, such as esophageal carcinoma or trauma, or following certain surgical procedures
Clinical Manifestations
Diagnostic Evaluation
-
Barium study of the esophagus outlines hernia.
-
Endoscopic examination visualizes defect.
Management
-
Elevation of head of bed (6 to 8 inches [15 to 20 cm]) to reduce nighttime reflux.
-
Antacid therapy to neutralize gastric acid.
-
H2-receptor antagonist (cimetidine, ranitidine) if patient has esophagitis.
-
Surgical repair of hernia if symptoms are severe.
Complications
-
Aspiration of reflux contents
-
Ulceration, hemorrhage
-
Gastritis
-
Stricture
-
Incarceration of the portion of the stomach in the chest
Nursing Interventions and Patient Education
-
Instruct patient on the prevention of reflux of gastric contents into esophagus by:
-
Eating smaller meals.
-
Avoiding stimulation of gastric secretions by omitting caffeine and alcohol.
-
Refraining from smoking.
-
Avoiding fatty foods: promote reflux and delay gastric emptying.
-
Refraining from lying down for at least 1 hour after meals.
-
Losing weight, if obese.
-
Avoiding bending from the waist and/or wearing tight-fitting clothes.
-
-
Advise patient to report to health care facility immediately for the onset of acute chest pain, which may indicate incarceration of a large paraesophageal hernia.